Can fasting or calorie restriction help my body fight cancer? Could it also help cancer treatment be more effective?
Claim: Fasting and calorie restriction (CR) can slow and even stop the progression of cancer, kill cancer cells, boost the immune system, and significantly improve the effectiveness of chemotherapy and radiation therapy.
What is It?
First, let’s define CR versus fasting and explore the history around these two practices. Calorie restriction means limiting the consumption of food, without resulting in malnutrition, to less than what an organism would eat if given free access. Fasting on the other hand is voluntarily not eating any food for varying lengths of time. Fasting has been used as a therapy for many different conditions as well as a part of spiritual/religious practices throughout history.
Table 1. Definitions of Calorie Restriction and Fasting
| Term | Definition |
| Calorie Restriction | 20-40% reduction in calorie intake over a long period of time (1200 calories for women vs 1400 calories for men per day) |
| Intermittent Calorie Restriction | 50-70% reduction in calorie intake for short periods of time (600-1000 calories per day) |
| Fasting | Complete avoidance of calorie intake for anywhere from 1 day to several weeks |
| Intermittent Fasting | Complete avoidance of calorie intake for 16-18 hours daily or alternating a fasting day with a normal energy intake day |
Fasting is one of the oldest therapies in medicine. Many renowned physicians throughout history and many of the oldest healing systems have recommended fasting as an integral method of healing and prevention. Hippocrates believed that fasting enabled the body to heal itself.
Fasting is a part of most spiritual traditions in the world, including Christianity, Hinduism, Judaism, Buddhism, and Islam. Many of history’s great spiritual leaders fasted for mental and spiritual clarity, including Jesus, Buddha, and Mohammed. In one of the more well-known political acts of the last century, the Indian leader Mahatma Gandhi fasted for 21 days to promote peace.
Humans have encountered many long periods of famine in their history, and although it is influenced by many factors, it appears that most humans can survive for over a month on water alone. Historically, most organisms have lived in environments of fluctuating food availability, during which periods of starvation were a commonly encountered condition, and evolution has selected for organisms that are able to withstand starvation.
What is the Evidence?
There has been over 100 years of research looking at the role of calorie restriction in relation to the possibility of prolonging life. While most of this research has been on animals, a modest amount of information on humans has accumulated that indicate a protective effect against secondary aging. Specifically, risk factors for atherosclerosis and diabetes are markedly reduced in humans following CR, along with inflammatory markers, like C-reactive protein (CRP) and tumor necrosis factor (TNF) (Holloszy). We will be diving into the research specifically on the topics of calorie restriction, fasting and cancer. We’ll start by taking a look at the physiological mechanisms being studied and then move on to explore some interesting human studies.
Biology
Adaptation to starvation requires an organism to divert energy into multiple protective systems to minimize the damage that would reduce fitness. It is thought that these systems can also prolong life and decrease cancer risk. According to a review by Drs. Longo and Fontana of the University of Southern California, CR without malnutrition is the most potent and reproducible physiological intervention for increasing lifespan and protecting against cancer in mammals (1). CR reduces the levels of a number of anabolic hormones, growth factors and inflammatory cytokines, reduces oxidative stress and cell proliferation, enhances autophagy (cell destruction) and several DNA repair processes (1). (See Figure 1)
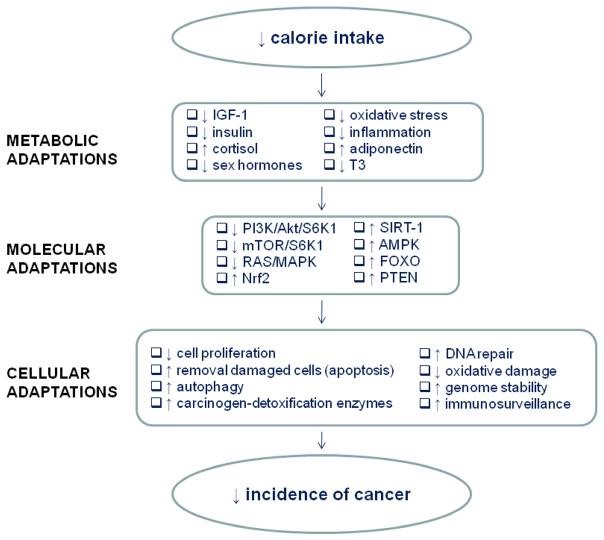
Figure 1. Mechanisms for cancer prevention by calorie restriction cause several key metabolic/hormonal adaptations that alter the expression of several genes and signaling pathways, which produce major cellular adaptations that result in a reduced cancer incidence (1).
One of the key metabolic factors in the above list is insulin-like growth factor-1 (IGF-1). We cover the role of IGF-1 and cancer in both our Sugar and Low Carbohydrate Diet sections of this website. An interesting observation that Dr. Longo makes is that CR was only successful at lowering IGF-1 when the protein intake was also restricted (1). High protein intake, or a positive nitrogen balance, was associated with increased IGF-1. This is an important point as many cancer patients are told to increase their protein intake during treatment; this recommendation may need to be re-examined.
There are several concerns with CR. One is that it requires weeks, or even months, to be effective at creating the metabolic changes described above. Another concern is that it generally results in chronic weight loss. At least a 15% weight loss is expected with moderate (20%) CR (2). This could be desirable for people who are overweight, but for those at a healthy weight or those that are already at a marginal weight, this could result in becoming underweight and malnourished.
Another option then for CR could be intermittent CR or intermittent fasting, which may actually be more protective and less concerning for weight loss. It may result in greater decreases in fat storage, IGF-1, and cell proliferation, while increasing insulin sensitivity and adiponectin levels (3). These results come from the earliest studies of spontaneous mammary tumor models on rodents, which compared fasting on alternate days versus fasting for 2-3 day periods each week. Both approaches reduce tumor incidence by 40-80% compared to ad lib feeding in a number of models, but the effects were most evident using alternate-day intermittent fasting (3).
There are three metabolic stages during food deprivation or fasting. These are described in greater detail by Dr. Longo and Dr. Lee (4). The first phase can last for 10 or more hours and uses up glycogen stores for energy. Once glycogen stores have been depleted, the body turns to glycerol and free fatty acids released from adipose tissue. These nutrients create ketones, which the body and brain can then use for energy. This phase can last for several weeks, depending on the size and health of the person.
In addition to fasting, a ketogenic diet, as described in our Low Carbohydrate Diet section, can also switch the energy source from glucose to fatty acids. Theoretically, the ketogenic diet can be sustained for longer, as calories and other essential nutrients continue to be consumed; although the tolerability of the diet may be challenging for some patients. With fasting, once the fat reserves are exhausted, muscle breakdown begins in order to continue to fuel gluconeogenesis.
Unlike CR, fasting induces changes associated with cellular protection to actually protect against weight loss initially and increases protection from oxidative stress (4). Fasting results in a more significant drop in insulin levels, as well as an increase in insulin sensitivity in a shorter amount of time compared to CR. Given that insulin levels play a role in cancer risk, these differences are potentially clinically important.
Furthermore, it is theorized that cancer cells do not respond to the protective signals generated by fasting, thus leaving them vulnerable to both the immune system and cancer treatment. This process is known as differential stress resistance (DSR). Short-term starvation (STS), fasting for 48 hours, causes a rapid switch of cells to a protected mode, which is capable of protecting mammalian cells and mice from various toxins, including chemotherapy (5).
Research Studies
The first scientific paper reporting that CR inhibited the growth of tumors transplanted into mice was published by Carlo Moreschi in 1909 (1). Since then, a large body of work has established that CR reduces the progression of tumors in various animal models. Additional research in both rodents and monkeys have shown that when CR was started by 12 months of age, lifespan was increased and incidence of spontaneous cancers was reduced by 50% (7). Although most cancer cells do seem to be sensitive to CR, there are some cells that carry mutations that make them resistant to CR. This suggests that the efficacy of CR may be limited to certain cancers (8). Human studies have to date been limited; however, there are some interesting outcomes related to cancer risk reduction and reducing treatment-related side effects.
Risk Reduction and Tumor Regression
In 2014, Longo and colleagues demonstrated that fasting caused “old” immune cells to die in mice, which were replaced by stem cells as soon as the subjects recommenced eating. They concluded that a 3-day fast could help regenerate a strong immune system (9). They also demonstrated that a 48-hour fast in mice slowed the growth and spread of five out of the eight cancers studied. They showed that the combination of fasting cycles with chemotherapy was more effective than chemotherapy alone in all cancers studied (6). As these were all animal studies, and it is unknown if humans would have the same benefit; however, several active clinical trials are studying the effect of calorie restriction or fasting on cancer.
A 2007 study (n=16) showed that alternate-day fasting, in which one day calories stayed at 400 for women and 600 for men, and the other day was unregulated, reduced blood levels of glucose, insulin and IGF-1 with a long-term risk reduction of chronic diseases including cancer, diabetes, and cardiovascular disease (10). Two calorie restriction studies, one that included women at moderately increased risk of breast cancer (n = 19) and the other that included newly diagnosed pancreatic cancer patients (n = 19) showed a decrease in serum markers (IGF, stearoyl-CoA desaturase, fatty acid desaturase, and aldolase C), possibly related to cancer risk and prognosis (11, 12).
A recent study analyzed data from the Women’s Healthy Eating and Living study and found that breast cancer survivors who didn’t eat for at least 13 hours overnight had a 36% reduction in the risk of recurrence and were 21% less likely to experience breast cancer related mortality (13). The proposed mechanism for this finding is thought to be related to better glycemic control resulting in protection against carcinogenesis. Each 2-hour increase in nightly fasting was linked to progressively lower hemoglobin A1C levels. This research is particularly interesting because it is a dietary strategy that most people could implement.
Protection from Treatment-Related Side Effects
Fasting may also protect patients against the harmful side effects of chemotherapy or radiation therapy. Fasting for up to five days, followed by a normal diet prior to treatment may reduce side effects from treatment, without causing chronic weight loss or interfering with the therapeutic effect of treatment (14). Older cancer patients (n=10), who voluntarily underwent short-term fasting before and/or after chemotherapy reported fewer side effects (15). A small study (n=6) reported a reduction in fatigue, weakness, and gastrointestinal side effects, compared to receiving chemotherapy without fasting (5). As shown in Figure 2, the trend for a reduction of many additional side effects was also reported by the group of patients who always fasted before chemotherapy.
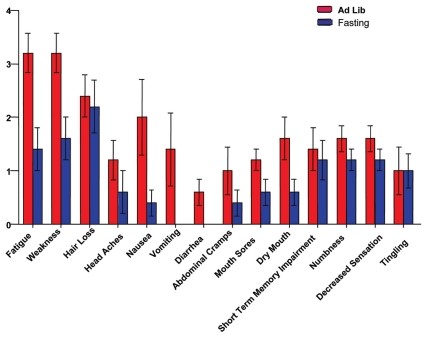
Figure 2. Average self-reported severity of symptoms in patients that received chemotherapy with or without fasting (5)
Safety
In a large cohort study of 2000 participants, fasting (350 kcal/day) was shown to be safe and actually beneficial to their chronic disease (rheumatic diseases, chronic pain syndrome, hypertension, metabolic syndrome) (16). The biggest concern with calorie restriction and fasting as it relates to cancer is weight loss. As discussed above, weight loss is actually less of a concern with short-term fasting than it is with long-term calorie restriction. For people who are overweight, this can be a positive side effect; however, for cancer patients who are already underweight or struggling to maintain their weight, additional weight loss may be detrimental and be a contraindication to fasting or CR. It is also worth mentioning that side effects, such as headache, light-headedness, nausea, or weakness, can occur when fasting longer than several days. Side effects, such as anemia or amenorrhea, can occur with fasting lasting several weeks. The longer the fast, the more important it is to take care in re-feeding. This phase needs to be gradual and incremental in order to prevent severe problems–or even death–coming off of a prolonged fast.
What is Our Recommendation?
Comparing the research between CR and fasting, fasting seems to provide more dramatic results and protection of healthy cells, without the risk of weight loss or immune suppression. Both CR and fasting are the subject of ongoing research, and definitive conclusions await the results of those studies. As mentioned above, it may not be appropriate for everyone, particularly those who are underweight or very ill, and should never be attempted without the supervision of qualified practitioners.
For general cancer prevention, it may be beneficial to add intermittent or short-term fasts in combination with a plant-based cancer prevention diet, as described in detail in the Dietary Approaches section of this website.
Here are some take-home tips from our literature review:
- In general, follow an anti-inflammatory diet with lots of colorful fruits, vegetables, beans, lentils, herbs and spices.
- Low to moderate carbohydrate intake with low glycemic starches
- Healthy fats at every meal, including good sources of Omega-3s
- Moderate protein intake of 3-4 ounces per meal from a combination of animal and plant proteins
- Lengthen the time between dinner and breakfast to allow for a longer overnight fast, with the goal of 13 or more hours, for example dinner by 6:00 pm and breakfast after 7:00 am.
- Short-term water fasts of 1-3 days to possibly help re-generate the immune system and increase cellular protection against oxidative stress. Working with a healthcare provider, you can determine how often it may be appropriate for you to engage in a fast.
- If you are a cancer patient, water fasting 2-3 days prior to treatment and up to one day following treatment to optimize the efficacy of treatment and reduce treatment-related side effects may be considered, but only under the supervision of a qualified practitioner.
References:
- Longo VD, Fontana L. Calorie restriction and cancer prevention: metabolic and molecular mechanisms. Trends in pharmacological sciences 2010;31:89-98.
- Racette SB, Das SK, Bhapkar M, et al. Approaches for quantifying energy intake and %calorie restriction during calorie restriction interventions in humans: the multicenter CALERIE study. American journal of physiology Endocrinology and metabolism 2012;302:E441-8.
- Harvie M, Wright C, Pegington M, et al. Intermittent dietary carbohydrate restriction enables weight loss and reduces breast cancer risk biomarkers. Cancer Research 2011;71.
- Lee C, Longo VD. Fasting vs dietary restriction in cellular protection and cancer treatment: from model organisms to patients. Oncogene 2011;30:3305-16.
- Raffaghello L, Safdie F, Bianchi G, Dorff T, Fontana L, Longo VD. Fasting and differential chemotherapy protection in patients. Cell cycle (Georgetown, Tex) 2010;9:4474-6.
- Lee C, Raffaghello L, Brandhorst S, et al. Fasting cycles retard growth of tumors and sensitize a range of cancer cell types to chemotherapy. Science translational medicine 2012;4:124ra27.
- Colman RJ, Anderson RM, Johnson SC, et al. Caloric restriction delays disease onset and mortality in rhesus monkeys. Science (New York, NY) 2009;325:201-4.
- Kalaany NY, Sabatini DM. Tumours with PI3K activation are resistant to dietary restriction. Nature 2009;458:725-31.
- Cheng CW, Adams GB, Perin L, et al. Prolonged fasting reduces IGF-1/PKA to promote hematopoietic-stem-cell-based regeneration and reverse immunosuppression. Cell stem cell 2014;14:810-23.
- Varady KA, Hellerstein MK. Alternate-day fasting and chronic disease prevention: a review of human and animal trials. The American journal of clinical nutrition 2007;86:7-13.
- Ong KR, Sims AH, Harvie M, et al. Biomarkers of dietary energy restriction in women at increased risk of breast cancer. Cancer prevention research (Philadelphia, Pa) 2009;2:720-31.
- Wright JL, Plymate S, D’Oria-Cameron A, et al. A study of caloric restriction versus standard diet in overweight men with newly diagnosed prostate cancer: a randomized controlled trial. Prostate 2013;73:1345-51.
- Marinac CR, Nelson SH, Breen CI, et al. Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA oncology 2016.
- Safdie F, Brandhorst S, Wei M, et al. Fasting enhances the response of glioma to chemo- and radiotherapy. PloS one 2012;7:e44603.
- Safdie FM, Dorff T, Quinn D, et al. Fasting and cancer treatment in humans: A case series report. Aging 2009;1:988-1007.
- Michalsen A, Li C. Fasting therapy for treating and preventing disease – current state of evidence. Forschende Komplementarmedizin 2013;20:444-53.
from Hacker News https://ift.tt/2VoTPJx
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.